Spondylolysis:

This is the medical term used to describe the presence of a “defect” or stress fracture in the posterior arch of the vertebra (see figure, arrow). It occurs at the lumbo-sacral junction (L5/S1) in about 85% of cases. The remainder occur at the L4/5 level or above, and in about 20% of cases the defect is on one side only (unilateral).
Spondylolysis is not a congenital condition and has never been identified in a newborn infant, or a child who has not started to walk. Defects usually develop as a stress fracture in individuals predisposed to the condition, due to the shape or orientation of the bones at the base of your spine.
There is an increased incidence in people who take part in certain physical or sporting activities such as female gymnasts, fast bowlers in cricket, and weight lifters. These types of people are also more likely to experience symptoms due to this condition.
Spondylolysis is evident in about 6% of the population, but only 10 to 15% of those individuals who have a spondylolysis develop symptoms of low back pain that can be attributed to this process. The remainder are considered an incidental finding.
A spondylolysis will usually develop in late childhood or early adolescence, and if symptomatic at this stage your specialist may recommend the avoidance of activities that aggravate the condition and cause discomfort. In some cases a brace is used to reduce movement at the level of the spondylolysis if the defect is thought to be of recent onset in the hope that the defect or stress fracture will heal. Healing is however not always achieved, but despite this, symptoms will usually settle within six to twelve weeks.
Whether the defects heal or not, some modification in the way certain activities are performed is likely to be recommended in order to avoid a recurrence of symptoms. Individuals with this condition should also obtain advice from an appropriately qualified physiotherapist or physical trainer in order to develop a program of muscle toning activities to improve the muscular support of the area and decrease the risk of further symptoms.
Regular swimming is one way to improve fitness and the muscle tone of the trunk without placing undue stress on the spine. A Pilates exercise program may also be of assistance.
It is however common for these defects to become chronic, and remain evident throughout life, but there is no need to become alarmed if this occurs, as the majority of people who have a spondylolysis experience no more back pain than other members of the general population who do not have this condition.
In adults who have a spondylolysis, degenerative changes are often evident in the adjacent discs or facet joints, which are just as likely, if not more so, to be responsible for symptoms of back discomfort. It is therefore important for your specialist to identify the origin of your pain before recommending the appropriate course of treatment.
So, to put it simply a spondylolysis is usually an incidental finding on an x-ray or CT scan undertaken to assess back pain due to another cause.
Spondylolisthesis:
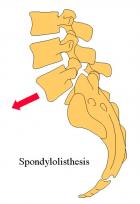
Spondylolisthesis is the term used to describe the presence of a spondylolysis where there has also been anterior translation of the vertebra with the lysis (usually L5), on the vertebra below (usually the sacrum).
In the majority of cases the degree of anterior translation is slight, but in approximately 20% of cases the displacement of the upper vertebra can be marked.
Progression of the “slip” usually occurs in early adolescence and is more common in girls than boys.
The development of a spondylolysis which then goes on to a spondylolisthesis is usually associated with significant low back pain, but in most cases the situation will stabilise and pain will settle. It is only where severe pain persists, or features of nerve root irritation or compression develop that surgical intervention is indicated at this stage.
In cases where symptoms resolve some activity modification may be required to reduce the risk of recurrent episodes of pain as outlined for spondylolysis. It is also important to maintain general fitness, and specifically the tone in the abdominal musculature.
If symptoms persist surgical intervention may be considered, and would usually take the form of a spinal fusion. However despite the often impressive x-ray appearance of this condition surgery of this type is required in less than 10% of cases.